ABILITY
|
What it is:
Ability refers to a wide range of physical, cognitive and/or emotional strengths and needs. It can include your physical and mental health, as well as your learning strengths and challenges. |
Remember:
When we talk about identity, disability tends to come up more than ability. However, ability is part of everyone’s identity, not just the identities of people with disabilities. We each have our own constellation of strengths and needs. And at some point in our lives, nearly everyone experiences a disability or learning difference even if it is not permanent or significant. The “medical model” of disability frames disability as an individual medical issue. However, most disability advocates today subscribe to the idea that disability is socially constructed. In other words, what we see as a “disability” depends on our societal expectations of what a healthy person is. It is society that creates, or at least contributes to, disability by excluding or refusing to accommodate those with different physical, mental, or emotional needs. Additionally, utilizing a medical model may result in overlooking environmental issues contributing to a person’s struggles. Ability can be a matter of perspective. What may typically be considered a disability can be an ability in a different context. For example, while people with dyslexia may find reading challenging, they often excel in visual causal reasoning. “Disability” should not have negative connotations. It is important for people to disclose their disabilities so that they can access services and accommodations. Talking frankly about disability can reduce the stigma around it. |
|
Examples of Personal Modifiers:
|
|
FAQs
According to the Autism Awareness Centre, “Neurodiversity is the concept that humans don’t come in a one-size-fits-all neurologically ‘normal’ package. Instead, it recognizes that all variations of human neurological function need to be respected as just another way of being, and that neurological differences like autism and ADHD are the result of normal / natural variations in the human genome.” Through the lens of neurodiversity, disability is not a catalogue of deficits but rather a different and equality legitimate way of being human. The term is most commonly used in the autism community. For example, in his book Uniquely Human: A Different Way of Seeing Autism, Dr. Barry M. Prizant argues that “the most successful approaches to autism don’t aim at fixing a person by eliminating symptoms, but rather seeking to understand the individual’s experience and what underlies the behavior.”
Increasingly, neurodiversity is seen as a benefit to our society. For example, see this Harvard Business Review article
discussing the competitive advantages of a neurodiverse workforce.
This image below has sometimes been used in conjunction with neurodiversity, to show that different people experience the same situation/image/conversation/class/book/etc. in different ways. What do you first see in this image: a bird, or a rabbit? Can you see both at the same time? How does this become an analogy for neurodiversity?
Neurodiversity (and specifically autism awareness) often uses a rainbow infinity symbol (see below) to symbolize the diversity present within the autism spectrum, as well as the greater neurodiversity movement.
When is a disability really an ability?
(Thank you to Katelyn Parisi, Laura Albert, and Emily Gray for the following response!)
Because disability is socially constructed, many “disabilities” can be abilities if you look at them from another perspective. Read the following articles for a few examples:
- Geology professor Dr. Michele Cooke writes about “deaf gain,” or the value that deaf and hard-of-hearing people add to their communities.
- This Forbes article entitled “The Benefits of Recruiting Employees with Autism Spectrum Disorder”
- This Harvard Business Review article entitled “Neurodiversity as a Competitive Advantage”
- This New York Times article entitled “The Autism Advantage”
- Another New York Times article entitled “Open Office: What Happens When People Who Have Trouble Fitting into a Traditional Workplace Have One Designed Just for Them?”
- Both Scientific American and Wired Magazine explore the cognitive strengths that often come with dyslexia.
Also check out this list of notable individuals with disabilities:
|
Art/Music/Entertainment Michelangelo - limited mobility in his hands, autism,
Italian sculptor, painter, architect, and poet of the High Renaissance Van Gogh - epilepsy and bipolar disorder, Dutch
post-impressionist painter Matisse - required the use of a wheelchair after
surgery for cancer, French artist (draughtsman, painter, sculptor,
printmaker) Beethoven - deafness, German composer and pianist Judith Scott - Down syndrome, American fiber sculptor Michael J Fox - Parkinson’s disease, Canadian-American
actor Stevie Wonder - blindness, America singer, songwriter,
musician Tom Cruise - dyslexia, American actor and producer (Top
Gun, Mission Impossible) Millie Bobby Brown - partial hearing loss, English actress
(Stranger Things) Edward Barbanell - Down syndrome, American actor and comedian Mariah Carey - bipolar, American singer and songwriter Anthony Hopkins- Autism SpectrumDisorder |
|
|
Math/Science Stephen Hawking - ALS, theoretical
physicist/mathematician Thomas Edison - deafness, American Inventor, light bulb Temple Grandin - autism, animal science, inventor of “hug
box” Albert Einstein - dyslexia, German physicist/mathematician,
theory of relativity Wanda Diaz Merced - blindness, Astronomer Alexander Graham Bell - learning disability, inventor of the
telephone Farida Bedwei - Cerebral Palsy, Ghanaian software engineer, co-founder of Logiciel |
Literature Stephen Hawking - ALS, author Sherman Alexie - bipolar, American novelist, short story
writer, poet, filmmaker F. Scott Fitzgerald - dyslexia, American fiction writer Dav Pilkey - dyslexia and ADHD, American author and
illustrator of children’s literature, best known for Captain Underpants
series |
|
History Franklin D. Roosevelt - Polio, 32nd president of United States Helen Keller - deafness and blindness, American political
activist, first deaf-blind person to earn a Bachelor of Arts degree |
|
How should I talk about disability?
Here are some guidelines from Kids as Self Advocates (KASA):
- Do not refer to a person's disability unless it is relevant. For example, don’t ask “What’s wrong with you?” or refer to the “girl in the wheelchair”.
- Use "disability" rather than "handicap" to refer to a person's disability. When talking about or referring to parking spaces or bathroom stalls used by people with disabilities say "accessible" or “disabled” parking or “accessible” or “disabled” access stall.
- Never use "cripple/crippled" when talking about disability in general or the person.
- Don't portray people with disabilities as overly courageous, brave, special, or superhuman. This makes it sound like it is unusual for people with disabilities to have talents, skills or to live life like everyone else.
- Don't use "normal" to describe people who don't have disabilities. It is better to say "people without disabilities” if necessary to make comparisons.
What other language is okay to use? What language should I avoid?
It is usually best to use “person-first” language. For example, say “people with disabilities” or “people without disabilities” or “person with [specific disability]” or “person without [specific disability].” For more detail, check out:
- This helpful chart of inappropriate and appropriate language from USAID
- This blogger’s glossary of ableist words and phrases
- This blogger’s exploration of the “language of disability”
"People-first" or "person-first" language is a way of describing disability that involves putting the word "person" or "people" before the word "disability" or the name of a disability, rather than placing the disability first and using it as an adjective. Some examples of people-first language might include saying "person with a disability," "woman with cerebral palsy," and "man with an intellectual disability." The purpose of people-first language is to promote the idea that someone's disability label is just a disability label—not the defining characteristic of the entire individual. Many guides on disability language and etiquette may likely emphasize using person-first language, except, perhaps, when discussing certain disability cultural groups that explicitly describe themselves with disability-first language. Thus, while it is generally a safe bet to use people-first language, there are members of certain disability groups in the US who prefer not to use it, such as the American Deaf community and a number of Autistic people/Autistics. The basic reason behind members of these groups' dislike for the application of people-first language to themselves is that they consider their disabilities to be inseparable parts of who they are. Using person-first language, some also argue, makes the disability into something negative, which can and should be separated from the person.
Some, but not all, people with disabilities/disabled people dislike the term “differently abled.” Here’s an explanation of the term from the National Center on Disability and Journalism:This term came into vogue in the 1990s as an alternative to “disabled,” “handicapped” or “mentally retarded.” Currently, it is not considered appropriate (and for many, never was). Some consider it condescending, offensive or simply a way of avoiding talking about disability. Others prefer it to “disabled” because "dis" means "not," which means that "disabled" means "not able." But particularly when it comes to referring to individuals, "differently abled" is problematic. As some advocates observe, we are all differently abled.
Some final thoughts from KASA:Remember to also take into consideration differences in culture as well as age. What is “OK” for some folks, is not “OK” for others. If you are unsure, please ask the person how she or he describes himself or herself. When in doubt, call the person by his or her NAME.
For more details, check out the United Spinal Association’s guide to “Disability Etiquette.”
How can I talk to my students about ability?
(Thank you to Katelyn Parisi, Laura Albert, and Emily Gray for the following response!)
Including ability in the conversation about identity can help students recognize that differing abilities is part of being human and fight some of the stigma around disability.
One way to start the conversation about ability is to have a survey or activity around personal strengths and needs. This can be done individually or in small groups. The activity can serve a variety of purposes including getting to know your students better, students getting to know each other better, students considering aspects of their own identity, and students getting to know the teacher better.
Sample questions:
- What are your strengths? Talents?
- What are you proud of?
- What skills come easily to you?
- What is your learning style?
- In what areas are you strong?
- What areas would you like to improve?
- What skills are difficult for you?
- What do you struggle with?
- What are your goals?
- How can teachers help you succeed?
Why do some students get accommodations?
As the International Dyslexia Association writes, accommodations “change the way students access information and demonstrate their knowledge, skills, and abilities; they do not change academic standards or expectations.” The Association continues with, “accommodations are adjustments made to allow a student to demonstrate knowledge, skills, and abilities without lowering learning or performance expectations and without changing what is being measured (e.g., providing text in audio-format when academic knowledge [e.g., history, biology, literature] is the target skill being measured). Accommodations do not change the content of instruction, give students an unfair advantage, or change the skills or knowledge that a test measures. Accommodations make it possible for students with dyslexia [or another disability] to demonstrate their learning without being hindered by their disabilities.” Also, note that accommodations are not the same as modifications; examples of modifications would be less content or easier questions.
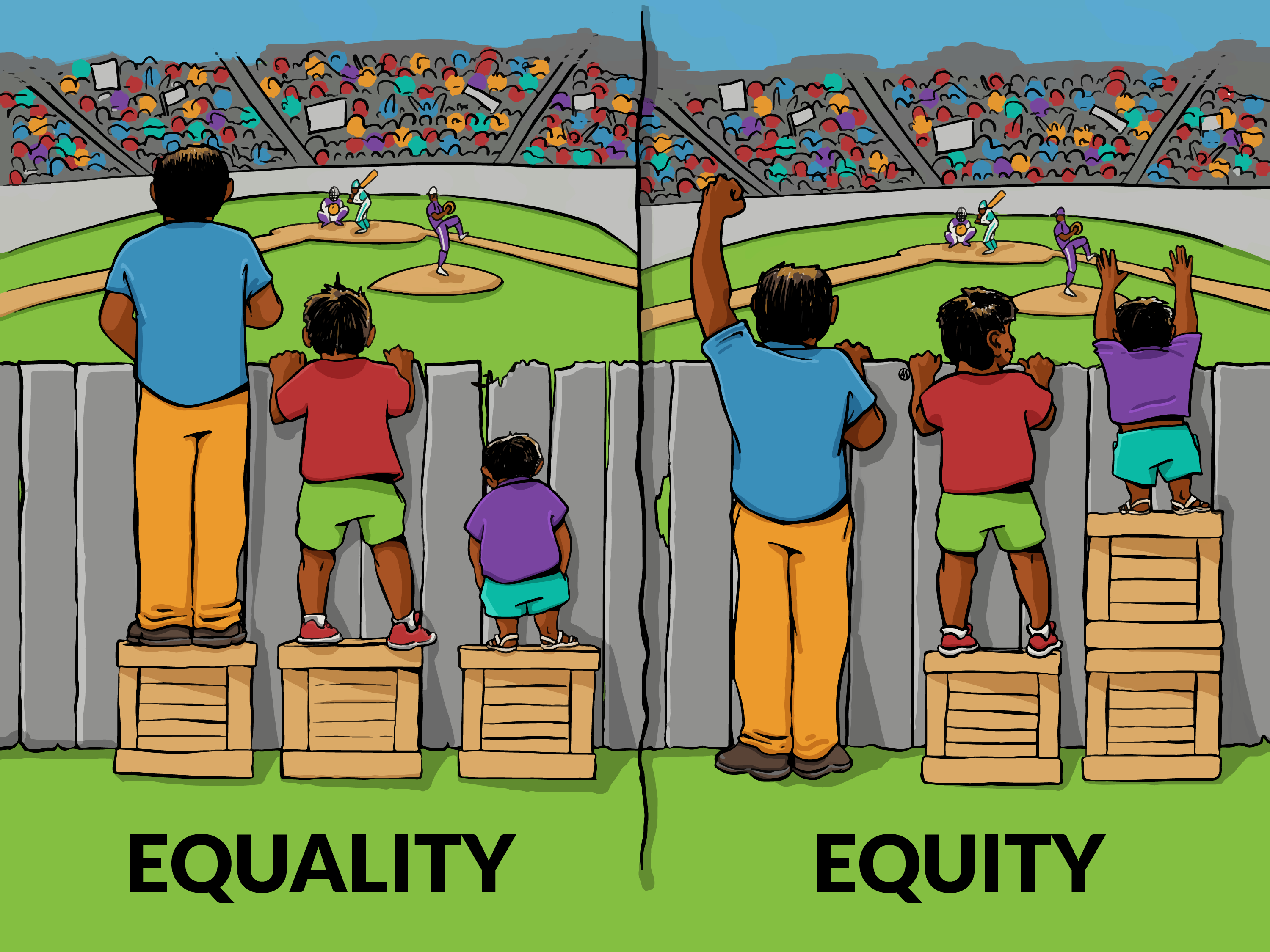
For some, it may be helpful to think of a particular accommodation as eyeglasses. Just as some people need eyeglasses in order to see clearly, others need classroom-based accommodations in order to effectively demonstrate what they know. We wouldn’t consider depriving a person of glasses, nor would we consider giving eyeglasses to everyone -- regardless of their vision. Similarly, we wouldn’t consider depriving a person of necessary accommodations, nor would we consider giving a specific classroom-based accommodation to everyone -- regardless of their ability/disability. Eyeglasses and classroom-based accommodations both help to provide more equity in the classroom, as shown by the right-hand side of the graphic below.
The graphic below from the Interaction Institute for Social Change is also a helpful reminder of the differences between equality and equity, and that fair does not mean equal.
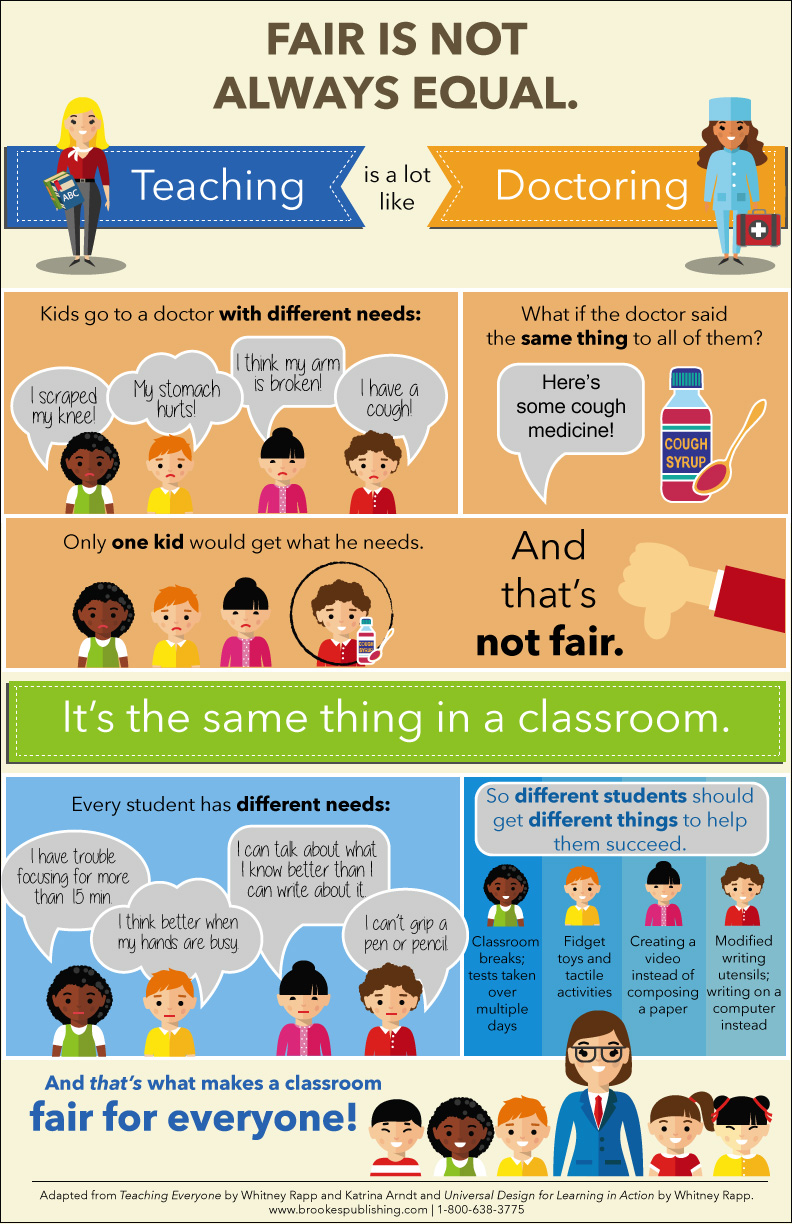
The following image builds upon the idea that fair does not mean equal, when it comes to both responses from a doctor and responses from a teacher. You can request a free poster of this image here.
What is “disability identity”?
According to the American Psychological Association, disability identity “refers to possessing a positive sense of self and feelings of connection to, or solidarity with, the disability community. A coherent disability identity is believed to help individuals adapt to disability, including navigating related social stresses and daily hassles.”
Read more about disability identity development here.
According to the Mayo Clinic, “Attention-deficit/hyperactivity disorder (ADHD) is a chronic condition that affects millions of children and often continues into adulthood. ADHD includes a combination of persistent problems, such as difficulty sustaining attention, hyperactivity and impulsive behavior.” As discussed in this article, some people with ADHD experience hyperfocusing, where a person experiences “intense concentration on a single interest or project for an extended period of time,” and may lose track of important relationships or situations in the surrounding environment. This article continues by quoting Dr. Kathleen Nadeau, who explains “People who think ADHD means having a short attention span misunderstand what ADHD is...a better way to look at it is that people with ADHD have a dysregulated attention system.”
For a person to receive a diagnosis of ADHD, these symptoms must be severe enough to interfere with everyday functioning. Some people use the term ADD to refer to ADHD without the hyperactivity, but the American Psychiatric Association (APA) only recognizes ADHD as a diagnosis. Most doctors now consider ADD to be an outdated term. What was once called ADD is now one of the types of ADHD, predominantly inattentive ADHD. The other two types are predominantly hyperactive-impulsive ADHD and combined ADHD. The latter is the most common type in the United States. According to the CDC, in 2016, 6.1 million U.S. children aged 2-17 years had been diagnosed with ADHD. They also estimated that approximately 1 out of every 20 U.S. children is taking prescribed ADHD medication.
According to The Cleveland Clinic, “The prevalence of ADHD increased 42% from 2003 to 2011, with increases in nearly all demographic groups in the United States regardless of race, sex, and socioeconomic status… Such data have sparked criticism, with some saying that ADHD is overdiagnosed, others saying it is underdiagnosed, and most agreeing that it is misdiagnosed. Changing definitions of ADHD may have had a small effect on the increase in prevalence, but the change is more likely a result of heightened awareness and recognition of symptoms. Even so, guidelines for diagnosing ADHD are still not rigorously applied, contributing to misdiagnosis. For example, in a study of 50 pediatric practices, only half of clinicians said they followed diagnostic guidelines to determine symptom criteria from at least 2 sources and across 2 settings, yet nearly all (93%) reported immediately prescribing medications for treatment.”
This Harvard Health Blog post about Alan Shwartz’s book ADHD Nation: Children, Doctors, Big Pharma, and the Making of an American Epidemic summarizes it this way: “Experts estimate that 5% is a realistic upper limit of children with the disorder, but in many areas of the country... up to 33% of white boys are diagnosed with ADHD.” On the other hand, “many children are appropriately diagnosed with ADHD and... a subset of these children will benefit from stimulants.”
What is autism? What is the autism spectrum?
Autism is a group of development disorders affecting communication and behavior. There is a very wide range in terms of both type and severity of characteristics, which is why autism is on a spectrum. There is more information here, as published by the National Institute of Mental Health. As the CDC writes, “autism spectrum disorder (ASD) is a developmental disability that can cause significant social, communication and behavioral challenges. There is often nothing about how people with ASD look that sets them apart from other people, but people with ASD may communicate, interact, behave, and learn in ways that are different from most other people. The learning, thinking, and problem-solving abilities of people with ASD can range from gifted to severely challenged. Some people with ASD need a lot of help in their daily lives; others need less. A diagnosis of ASD now includes several conditions that used to be diagnosed separately: autistic disorder, pervasive developmental disorder not otherwise specified (PDD-NOS), and Asperger syndrome. These conditions are now all called autism spectrum disorder.”
What about Asperger syndrome? The term Asperger syndrome is no longer used in the medical community. According to Autism Speaks, “Asperger syndrome, or Asperger’s, is a previously used diagnosis on the autism spectrum. In 2013, it became part of one umbrella diagnosis of autism spectrum disorder (ASD) in the Diagnostic and Statistical Manual of Mental Disorders 5 (DSM-5). Typical to strong verbal language skills and intellectual ability distinguish Asperger syndrome from other forms of autism.”
What are language-based learning disabilities? What is dyslexia?
As the Landmark School writes, language-based learning disabilities (LBLD’s), such as dyslexia, affect “age-appropriate reading, spelling, and/or writing. Most people diagnosed with learning disabilities have average to superior intelligence. People with LBLDs can also struggle with speaking and listening. LBLDs fall under the broader umbrella of Specific Learning Disability (SLD).”
As the Yale Center for Dyslexia and Creativity writes, “Dyslexia is defined as an unexpected difficulty in learning to read. Dyslexia takes away an individual’s ability to read quickly and automatically, and to retrieve spoken words easily, but it does not dampen their creativity and ingenuity.
“Dyslexic children and adults struggle to read fluently, spell words correctly and learn a second language, among other challenges. But these difficulties have no connection to their overall intelligence. In fact, dyslexia is an unexpected difficulty in reading in an individual who has the intelligence to be a much better reader. While people with dyslexia are slow readers, they often, paradoxically, are very fast and creative thinkers with strong reasoning abilities.
“Dyslexia is also very common, affecting 20 percent of the population and representing 80-90 percent of all those with learning disabilities. Scientific research shows differences in brain connectivity between dyslexic and typical reading children, providing a neurological basis for why reading fluently is a struggle for those with dyslexia.
“Dyslexia can’t be ‘cured’ – it is lifelong. But with the right supports, dyslexic individuals can become highly successful students and adults.”
The International Dyslexia Association published this list of common questions (and answers) about dyslexia.
How does the school classify different disabilities?
The following is an abbreviated version of a section from the PSB Special Education Standard Operating Procedure Manual, which outlines the disability categories the district recognizes, according to federal law:
Autism - A developmental disability significantly affecting verbal and nonverbal communication and social interaction.
Developmental Delay - The learning capacity of a young child (3-9 years old) is significantly limited, impaired, or delayed and is exhibited by difficulties in one or more of the following areas: receptive and/or expressive language; cognitive abilities; physical functioning; social, emotional, or adaptive functioning; and/or self-help skills.
Intellectual Impairment - The permanent capacity for performing cognitive tasks, functions, or problem solving is significantly limited or impaired and is exhibited by more than one of the following: a slower rate of learning; disorganized patterns of learning; difficulty with adaptive behavior; and/or difficulty understanding abstract concepts.
Sensory - The term shall include the following:
- Hearing
- Vision
- Deaf-Blind
Neurological - The capacity of the nervous system is limited or impaired with difficulties exhibited in one or more of the following areas: the use of memory, the control and use of cognitive functioning, sensory and motor skills, speech, language, organizational skills, information processing, affect, social skills, or basic life functions. The term includes students who have received a traumatic brain injury.
Emotional Impairment - The student exhibits one or more of the following characteristics over a long period of time and to a marked degree that adversely affects educational performance: an inability to learn that cannot be explained by intellectual, sensory, or health factors; an inability to build or maintain satisfactory interpersonal relationships with peers and teachers; inappropriate types of behavior or feelings under normal circumstances; a general pervasive mood of unhappiness or depression; or a tendency to develop physical symptoms or fears associated with personal or school problems.
Communication Impairments - The capacity to use expressive and/or receptive language is significantly limited, impaired, or delayed and is exhibited by difficulties in one or more of the following areas: speech, such as articulation and/or voice; conveying, understanding, or using spoken, written, or symbolic language. The term may include a student with impaired articulation, stuttering, language impairment, or voice impairment if such impairment adversely affects the student's educational performance.
Physical Impairment - The physical capacity to move, coordinate actions, or perform physical activities is significantly limited, impaired, or delayed and is exhibited by difficulties in one or more of the following areas: physical and motor tasks; independent movement; performing basic life functions. The term shall include severe orthopedic impairments or impairments caused by congenital anomaly, cerebral palsy, amputations, and fractures, if such impairment adversely affects a student's educational performance.
Health Impairment - A chronic or acute health problem such that the physiological capacity to function is significantly limited or impaired and results in one or more of the following: limited strength, vitality, or alertness, including a heightened alertness to environmental stimuli resulting in limited alertness with respect to the educational environment. The term shall include health impairments due to asthma, attention deficit disorder or attention deficit with hyperactivity disorder, diabetes, epilepsy, a heart condition, hemophilia, lead poisoning, leukemia, nephritis, rheumatic fever, and sickle cell anemia, if such health impairment adversely affects a student's educational performance.
Specific Learning Disability - The term means a disorder in one or more of the basic psychological processes involved in understanding or in using language, spoken or written, that may manifest itself in an imperfect ability to listen, think, speak, read, write, spell, or to do mathematical calculations. ...[It] includes conditions such as perceptual disabilities, brain injury, minimal brain dysfunction, dyslexia, and developmental aphasia.
What do I need to know about mental health?
Mental Health and the IEP
In Massachusetts, mental health issues that prevent a student from making adequate progress in school are categorized as emotional impairments. These are generally covered in the Plep B section of an IEP.
Regarding emotional impairments, the Massachusetts Department of Education writes:
As defined under federal law at 34 CFR §300.7, the student exhibits one or more of the following characteristics over a long period of time and to a marked degree that adversely affects educational performance:
- An inability to learn that cannot be explained by intellectual, sensory, or health factors.
- An inability to build or maintain satisfactory interpersonal relationships with peers and teachers.
- Inappropriate types of behavior or feelings under normal circumstances.
- A general pervasive mood of unhappiness or depression, or a tendency to develop physical symptoms or fears associated with personal or school problems.
When a Student Needs Mental Health Support
Whether or not a student is on an IEP, they may be struggling with a mental health issue that requires intervention or support. As an educator, here are some warning signs to watch for according to mentalhealth.gov:
- Feeling very sad or withdrawn for more than two weeks
- Seriously trying to harm oneself, or making plans to do so
- Sudden overwhelming fear for no reason, sometimes with a racing heart or fast breathing
- Involvement in many fights or desire to badly hurt others
- Severe out-of-control behavior that can hurt oneself or others
- Not eating, throwing up, or using laxatives to make oneself lose weight
- Intense worries or fears that get in the way of daily activities
- Extreme difficulty concentrating or staying still that puts the student in physical danger or causes problems in the classroom
- Repeated use of drugs or alcohol
- Severe mood swings that cause problems in relationships
- Drastic changes in the student's behavior or personality
Combating the Stigma in our Schools
Here are some ways to create a more open and positive culture around mental health and seeking support according to mentalhealth.gov:
- Educate parents and students on symptoms of and help for mental health problems
- Promote social and emotional competency and build resilience
- Help ensure a positive, safe school environment
- Teach and reinforce positive behaviors and decision-making
- Encourage helping others
- Encourage good physical health
- Help ensure access to school-based mental health supports
Hidden disabilities are ones that are not immediately apparent to others. This may include chronic pain, ADHD, trauma, PTSD, diabetes, sleep disorders, chronic illness, birth disorders, etc. Because these disabilities are not always obvious to others, they can be met with insensitivity both intentionally or unintentionally by those who make assumptions. It is important for educators and students to understand that not all disabilities are readily apparent. We do not always know the daily challenges that our students are facing, and this highlights the importance of building a safe, open, and inclusive school and classroom culture.
For a more complete list of hidden disability examples, please consult this paper from Disabled World.
What are some tips for reading an IEP?
In Brookline, all IEPs for your students can be found in Aspen in the documents tab. As IEPs are legal documents, at times it can be a bit of a challenge to parse through all of the language and information to pick out the gist of what a student needs to be successful in your class. Here are some tips for making sense of an IEP.
- Start with the vision statement. This approach avoids looking at a student from a deficit focused perspective and places more emphasis on what they can and want to do. Focusing first on the vision gives you a chance to get a more holistic view of the student and what they and their family are hoping for them in high school and beyond. Then, move on to the accommodations and goals.
- The goal of goals. Above all else, the goal of any IEP is to help students find success in school by developing more independence and ownership over their learning. Specific goals on a student’s IEP are designed to help them grow as a student, so that they can lead a fulfilling, productive life beyond high school. A challenge that students on IEPs can face is developing learned helplessness when they get too used to adults doing the thinking, organizing, planning, and advocating for them. Remember, our work toward accomplishing goals should (as much as possible) also be work toward fostering independence, a sense of accomplishment, and an awareness of personal learning styles and needs.
- Accommodations. When a class has a number of students on IEPs, consistently addressing each student’s accommodations can feel daunting. One easy way to make this task more management is to consider universal design in your curriculum with some of the most common accommodations such as graphic organizers and chunking of assignments.
- Print it out! Visually, Aspen is awful, and the IEP consists of a bunch of different tabs and sections. It can be much easier to read and digest when printed out or viewed as a PDF. When viewing an active IEP, click Reports → IEP Form → Run to print or save as a PDF. Another option is to take notes in a separate document, in a format that is easier for you to reference later.
- Ask for help! If a student is on an IEP, they have a liaison in charge of managing their case. This staff member is listed in the Attributes tab on the IEP. If you have any questions, comments, or concerns as you read and work to implement the IEP, please do not hesitate to reach out to the liaison for support. They often will know what other teachers are doing and can provide helpful tips and tricks. You’re not alone!
What is the history of disability rights and the Americans with Disabilities Act?
As with many other 20th century rights movements, the Disability Rights Movement was spearheaded by activists and allies who demanded societal changes. According to the National Park Service, these efforts throughout the late-1800’s and through the 1900’s involved grassroots organizing and community based groups such as the League of the Physically Handicapped, We are Not Alone, and the National Association of Retarded Children. Civil rights legislation as well as legislative acts in the 1970’s helped to combat workplace discrimination based on disability. In particular, the 1973 Rehabilitation Act and the 1975 Education of All Handicapped Children Act moved the fight forward. The latter mandated that disabled students have access to a public education. Legislative and community-based efforts continued throughout the 1980’s to increase legal protections, support, and access for people with disabilities. This multi-generational fight culminated with the Americans with Disabilities Act of 1990 and the amended version of 2008.
Americans With Disabilities Act (1990, amended 2008)
Source: ADA National Network
Title I - Employment
- Aims for equal employment opportunities for people with disabilities.
- Requires “reasonable” accommodations to be made by employers to allow employees to perform essential job functions.
- Applies to employers with 15 or more employees.
- Prohibits discrimination against people with disabilities in all state and local government agencies and programs.
- Applies to public transit as well, which was a contentious fight that delayed the original bill’s passage.
- Sets accessibility guidelines for construction and renovation.
- Prohibits discrimination by private businesses that serve the public against people with disabilities.
- Compels private businesses that serve the public to make reasonable accommodations in serving people with disabilities.
- Ensures that telecommunications services provide services to support communication for those with speech and hearing related disabilities.
- Ensures that all federally funded public service announcements are closed captioned.
- Explains how the ADA relates to other laws.
- Includes nuances regarding insurance, drugs, retaliation, etc.
- Lists conditions not to be considered disabilities.
What programs does Brookline High School offer for students with disabilities?
This page of our school website explains the special education programs we offer at the high school. BHS Special Education staff brings a wealth of varied and diverse backgrounds and knowledge to our institution, and they are happy to find time to meet with general educators to discuss ability, IEPs, etc. Please do not hesitate to reach out!
